It is 2:20 AM. I awoke Tuesday morning sick with a cold or the flu or somatic manifestations of despair–certainly not confined to the tax bill, but a sense of hopelessness that after Elizabeth MacDonough, Parliamentarian of the Senate, raised what is referred to colloquially as “the Byrd bath” before Christmas President Trump will sign a […]
Addison Court
Analysis: Limitations of disability housing design

Figure 1.1. Nadya Ludwig in her customary position watching the front door at Addison Court and greeting all 95 residents by name [1] ++++ Summary The generation born after the Second World War is commonly referred to as “The Baby Boom Generation.” The U.S. Census Bureau provides statistics on Baby Boomers not as helpful as one […]
Celebration of the Use of Virtual Reality to Improve Housing for the Elderly and Disabled
University Park, PA. On Tuesday, May 3, 2011 at 10a.m. Penn State’s Department of Architectural Engineering and its Smart Spaces Center for Adaptive Aging in Community celebrated progress made in a coordinated effort to reduce the cost of housing for Pennsylvania’s elderly and disabled residents today and in the future. The celebration took place at […]
Saving Medicare billions: Trying too hard can get in the way

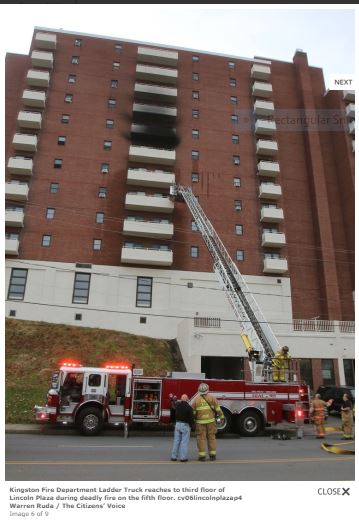
Today is Sunday, February 26, 2012. I took the photograph above last week. My apartment is within an eight-story building housing 90 low-income elderly and disabled individuals, an ambulance parks outside my window at least once a week. Sometimes my neighbors and I return. Sometimes, not. The cost for Medicare, Medicaid, and other services to […]
Lady Gaga: When you became disabled in “Paparazzi,” you needed cooler equipment

What I want you, oh dear Lady Gaga, as a disability and elderly rights advocate here in State College, Centre County, Pennsylvania to do is:
Sing for us at noon at the bingo parlor at Addison Court, 120 East Beaver Avenue, State College. Addison Court is an independent residence for the elderly and disabled. There are 90 of us. Several of us could use cheering up. We do not get to hear a lot of live music. Dazzle us.
Advocate for us. After Florida, Pennsylvania has more elderly residents than any other state in the union. Centre County is attracting large numbers of elderly residents who retire here. Yet the music venues in Downtown State College are closed to us because Downtown businessmen do not think it is worth their while to provide access so people using canes, wheelchairs, walkers, scooters, and power chairs can listen to live music.
Meanwhile, you could do a lot to increase opportunities for elderly and disabled residents of my town.
Come on by. Use your wealth to buy a front-wheel drive
or an Amigo real wheel drive
Virtual reality cuts costs and increases satisfaction

Put on your 3-D glasses The following appeared in HME News, the publication for the home medical industry, on July 26, 2011. This year and last, I asked the residents of Addison Court, the low-income apartment for disabled and elderly in State College where I live, to attend a demonstration at the Immersive Construction Lab, described […]
Saving Medicare billions: Trying too hard can get in the way

Memorial Note: November 13, 2011, Jack Seidner aged 93, my neighbor and friend at Addison Court, State College. PA, died while talking to his son who had called from Israel. He died at Centre Crest, an assistive care facility in Bellefonte, PA, 11 miles from Addison Court. Jack was a veteran of World War II […]
When I was treated for cancer 36 years ago, I wrote the following account:

[Note: I was diagnosed and treated for cancer in 1976 when I was 28 years old. This is how I described the experience when I was in the midst of my first round of radiation treatment.] […]